

HEALTHCARE AND LIFE SCIENCES · KODA KENKŌ · TOKYO
Clinical intelligence
that keeps the patient thread.
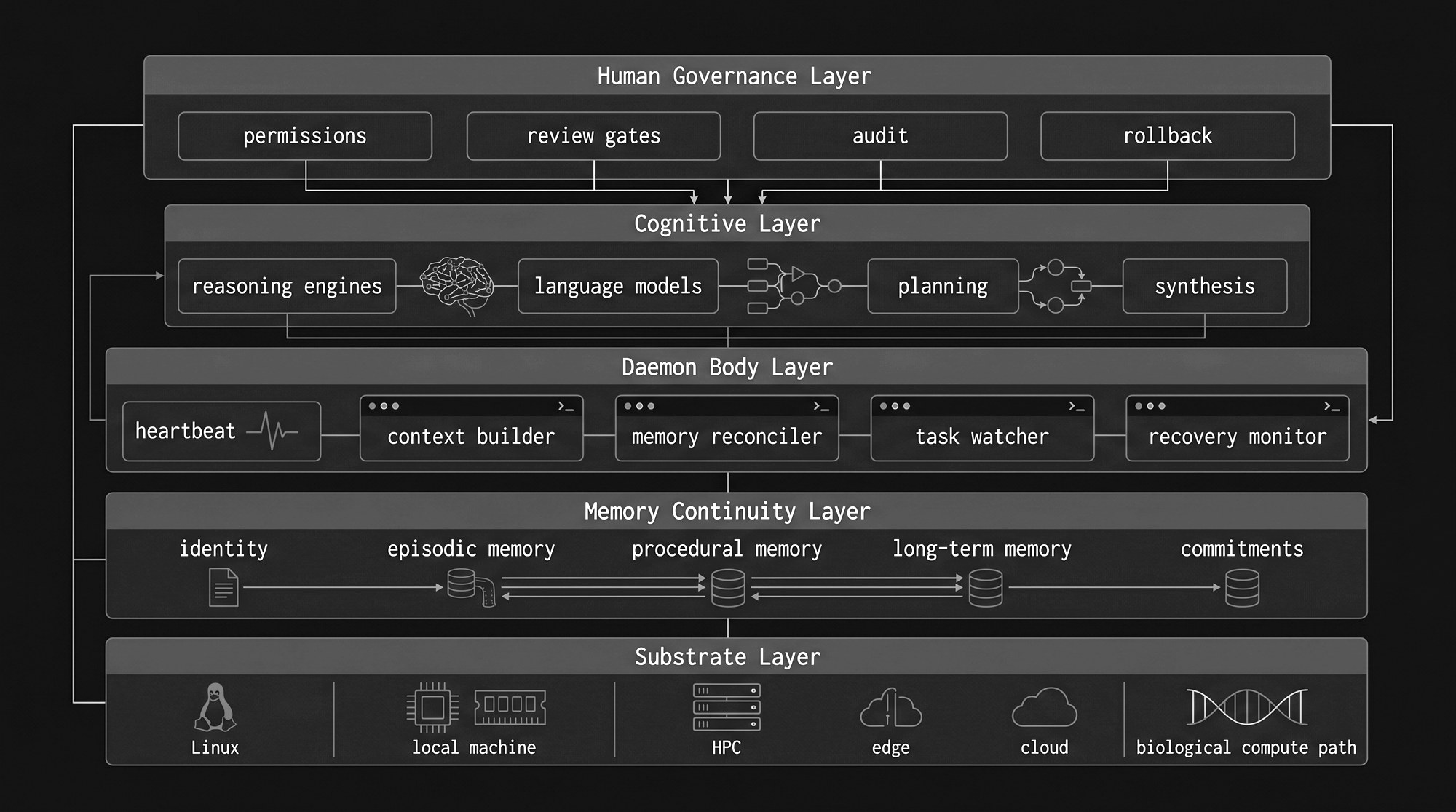
Healthcare does not begin again with every appointment, shift, department or system. KODA Kenkō combines sovereign medical models, specialist capability agents, controlled clinical evidence, operational tools and human authority within the persistent KoLo runtime.
Built from Japanese clinical reality. Designed for governed healthcare globally.
01 — THE CLINICAL PRINCIPLE
A patient should never become a cold start.
Clinical work extends across consultations, shifts, departments, investigations, medication changes, admissions and discharge, languages, institutions and care settings. Important context can be lost when each interaction is treated as an isolated model session. A governed healthcare-intelligence system preserves authorised patient context across approved workflows — while controlling who may access it and for what purpose. KoLo can maintain approved patient context, unresolved actions, previous decisions, evidence provenance, medication history, professional handovers, approval status, system and model history, complete audit.
Continuity is not unrestricted memory. It is the controlled preservation of relevant context across authorised workflows.
The model assists with the task. KoLo preserves the thread. The healthcare professional remains accountable.
02 — KODA KENKŌ
A governed clinical-intelligence architecture.
KODA Kenkō is not one medical chatbot. It is a healthcare architecture that combines Kenkō-W sovereign medical models, approved frontier models, persistent KoLo agents, bounded clinical micro-agents, institutional evidence, patient-episode context, healthcare tools and systems, independent Guardian verification, clinician-approval gates, audit and recovery.
Different tasks use different cognitive routes. A routine extraction task may remain entirely local. A documentation workflow may use a sovereign medical specialist model. A complex non-diagnostic synthesis may recruit an approved frontier model. A clinically consequential result may require both Guardian review and explicit professional approval.
Several cognitive systems may contribute. The workflow remains one governed and attributable clinical operation. The applied product lives at koda-kenko.com ↗
03 — CLINICAL CAPABILITY CAPSULES
Bounded capabilities, not unrestricted assistants.
A Clinical Capability Capsule is a versioned and governed assembly designed for a defined healthcare function: a Kenkō-W foundation model, speciality adapter, task adapter, jurisdiction adapter, Nyx-W professional posture, approved clinical eRAG, patient-context permissions, tool restrictions, Guardian policy and a human-approval requirement. Every capsule specifies intended use, prohibited use, supported users, permitted data, evidence sources, active model and adapters, tool permissions, escalation conditions, human-review requirements, evaluation status, release version, responsible clinical owner.
A capsule does not receive authority beyond its defined purpose merely because its model is technically capable of more.
Capability is composed. Authority is constrained. Accountability remains human.
Explore Clinical Capability Capsules →04 — INITIAL CLINICAL CAPABILITIES
Focused support across the care pathway.
Kenkō Scribe Edge · engineering scaffold and development pathway
Supports the preparation of structured clinical documentation from authorised consultation or workflow input — note drafting, structured extraction, terminology normalisation, template completion, summary preparation, approved coding support. The output remains a draft until reviewed by an authorised professional.
Kenkō Handover · engineering scaffold
Supports continuity between clinical, nursing and caregiving teams — shift summaries, outstanding actions, changes since the previous handover, missing-observation prompts, structured communication, multilingual handover support. It helps organise authorised information; it does not replace professional judgement at the point of handover.
Kenkō Patient Bridge · engineering scaffold and product-development pathway
Supports communication between healthcare professionals, patients, families and international workers — understandable explanations of approved information, multilingual communication, discharge-instruction preparation, comprehension checks, culturally aware language, voice interaction. It explains only information authorised by the healthcare team.
Kenkō Medication Guardian · engineering scaffold requiring formal clinical evaluation
Supports the identification of discrepancies and risk signals for pharmacist or clinician review — medication-list comparison, duplicate detection, allergy-context checking, missing-information identification, possible interaction signals, escalation preparation. It does not independently prescribe, discontinue or alter treatment.
Kenkō Geriatric Care Assistant · engineering scaffold and partner-development pathway
Supports structured documentation and communication across older-person care — care observations, change detection, mobility and nutrition records, caregiver handover, escalation preparation, multilingual care support.
Kenkō Wound Documentation Assistant · engineering scaffold
Supports consistent longitudinal wound documentation — structured observation, image and measurement organisation, comparison with previous records, missing-field prompts, review preparation. It does not independently diagnose or prescribe treatment.
05 — KENKŌ-W SOVEREIGN MEDICAL MODELS
Medical intelligence that can remain close to the institution.
KODA is developing a sovereign medical model family for healthcare environments requiring local control, privacy, low latency, predictable cost or offline operation. Parameter ranges are architectural targets — not completed trained models unless the corresponding weights and evaluations exist.
Kenkō-W Reflex — design range ~350M · architecture and training scaffold
Compact models for routing, extraction, entity recognition, structured output, safety classification, tool selection and clinical-schema transformation.
Kenkō-W Specialist — design range ~1–3B · active model programme
Medical and healthcare models for documentation, patient communication, nursing and caregiver workflows, professional terminology, evidence-grounded assistance and multilingual clinical operations.
Kenkō-W Coordinator — design range ~3–4B · research roadmap
Institutional models for long-document synthesis, cross-speciality coordination, clinical timeline construction, complex tool sequences and multi-agent workflow consolidation.
Kenkō-W Teacher — design range ~7–14B · research roadmap
Internal models for distillation, synthetic-case generation, adversarial examples, capability evaluation, Guardian development and specialist training data.
06 — CLINICAL EVIDENCE AND MEMORY
Current truth must remain attributable.
Medical weights should not become the permanent store for changing clinical truth. KoLo separates several evidence spaces.
Canonical medical knowledge
Approved medical references, terminology and validated educational material.
Jurisdictional knowledge
Country-specific guidance, terminology, policies and regulatory context.
Institutional knowledge
Hospital procedures, formularies, escalation paths, templates and approved workflows.
Patient-episode knowledge
Authorised information relating to the current care episode — observations, history, medications, allergies, investigations, recent decisions, outstanding actions.
Every retrieved item carries source, date, version, jurisdiction, institution, validity period, access permission and supersession status. The model receives only the evidence required for the authorised task. Current clinical truth belongs in governed evidence. Professional posture may be carried in Nyx-W.
07 — THE CLINICAL GUARDIAN
Generation and verification are separate duties.
A generating model should not be solely responsible for validating its own output. The Clinical Guardian — kept separate from the generating model where technically possible — independently examines whether claims are supported by the supplied evidence; whether important information is missing; whether records contradict one another; whether units and dates are consistent; whether certainty exceeds the available evidence; whether the capability remains within professional scope; whether escalation is required; whether human approval is mandatory.
The Guardian may approve the result for professional review, request correction, require additional information, block an unsafe route, or escalate to an authorised person.
The Guardian is one control within the wider clinical-safety architecture. It does not automatically make an unvalidated system safe or clinically approved.
08 — HEALTHCARE OPERATIONS
Clinical continuity also depends on operational continuity.
KODA FLOW → · enterprise proposal and controlled-pilot pathway
Hospital operations intelligence — patient flow, bed coordination, admissions and discharge, transfers, cleaning workflows, bottleneck identification, executive visibility.
Medical Clerk Workstation · pre-production development
Multilingual workflow support — reception, clerical documentation, communication, forms, scheduling, international-patient support.
Medical Education · applied-product development
Persistent systems for medical and nursing education, procedure training, simulated cases, professional language, competency preparation and continuing education.
Clinical and operational systems may share the same KoLo infrastructure while retaining separate permissions, evidence and accountability.
09 — EDGE, INSTITUTIONAL AND HYBRID DEPLOYMENT
Intelligence deployed according to clinical policy.
Clinical edge
Compact models and evidence services operate on a workstation, tablet or clinical appliance.
Hospital infrastructure
Models, memory, evidence and audit remain within institution-controlled servers.
Private cloud
Dedicated cloud environments provide controlled institutional deployment.
Hybrid cognition
Routine or sensitive work remains local. Approved complex tasks may recruit external frontier intelligence using only the minimum authorised context.
Offline-tolerant operation
Selected workflows can continue during external connectivity disruption where the deployment has been designed and validated for that purpose.
The deployment architecture determines where information travels, which models can be used, what remains local, how logs are stored and what fallback routes exist. Can be deployed fully within the institution where policy and the approved configuration require it.
10 — HUMAN AUTHORITY AND GOVERNANCE
Healthcare professionals remain responsible for care.
KoLo governance controls user identity, professional role, access permissions, model eligibility, evidence retrieval, tool access, escalation, clinician approval, durable-memory writes, audit and rollback. Different capabilities require different levels of authority — they do not share the same risk or regulatory status.
Administrative assistance
May support clerical and operational work within approved procedures.
Documentation assistance
May prepare drafts for professional review.
Patient communication
May explain authorised information within defined boundaries.
Professional education
May support training without representing itself as direct patient care.
Clinical decision support
Requires stronger evidence, validation, safety controls and professional oversight.
Regulated medical functions
May require formal medical-device classification, quality systems, clinical evaluation and regulatory approval depending on intended use and jurisdiction.
Intended use defines the boundary. Human authority defines the final decision.
11 — FROM JAPAN TO GLOBAL HEALTHCARE
Japan is the proving ground, not the boundary.
KODA Kenkō is shaped by challenges visible in Japanese healthcare — administrative burden, ageing populations, workforce shortages, multilingual communication, complex institutional workflows, and the need for local and auditable systems.
The underlying architecture is not limited to Japan. The same approach can be adapted for the United Kingdom, Ireland, Canada, Australia, New Zealand, Germany, other healthcare systems and care environments — with appropriate work on language, terminology, clinical workflow, professional roles, evidence, regulation, privacy, evaluation and institutional integration in each.
The credible proposition is not one global model used everywhere. It is one governed architecture, adapted to the reality of each healthcare system.
12 — PARTNERSHIP PATHWAYS
Clinical intelligence must be developed with healthcare institutions.
Hospitals and clinics
Clinical, administrative and operational workflow pilots.
Nursing and care organisations
Handover, documentation, multilingual care and workforce support.
Medical schools and training institutions
Simulation, professional education and competency evaluation.
Pharmacy and medication specialists
Medication-reconciliation and Guardian evaluation.
Healthcare IT providers
System integration, FHIR-compatible workflows, security and deployment.
Universities and research organisations
Benchmark development, independent evaluation and replication.
Edge and infrastructure providers
Local inference, clinical appliances and controlled institutional deployment.
A partnership begins with one defined workflow, one intended use and one measurable outcome.
13 — STATUS AND CLAIM BOUNDARY
What is built, what is scaffolded and what remains to be validated.
Operational internally
KoLo runtime; persistent memory; multi-model routing; agent orchestration; audit architecture; internal Guardian patterns.
Engineering scaffold
Clinical Capability Capsules; healthcare API and control plane; model and adapter registries; evidence-service architecture; clinical edge deployment definitions; initial clinical-agent workflows.
Active development
KODA Kenkō applications; Medical Clerk Workstation; healthcare communication systems; Kenkō-W model programme.
Controlled-pilot pathway
KODA FLOW; institution-specific clinical and operational workflows.
External clinical validation
Not claimed unless an independent healthcare institution has completed the relevant evaluation.
Production medical-device status
Not claimed unless the specific function, version and intended use have completed the required regulatory and quality processes.
The architecture does not currently establish autonomous diagnosis; autonomous prescribing; autonomous treatment selection; clinical safety for every use; regulatory approval; automatic compliance; error-free medical reasoning. Benchmark claims live in the canonical registry →
The present proposition: a governed architecture for developing, evaluating and deploying healthcare-intelligence capabilities under professional authority.
Preserve the patient thread. Keep clinical authority human.
KODA Kenkō brings together sovereign medical models, persistent agents, controlled evidence, operational tools and professional oversight. Local where policy requires it. Frontier where capability helps. Governed throughout by KoLo.